ALS genetics
for the neurology registrar
Evan Edmond
Neurology ST4
structure
- Is ALS genetic?
- C9orf72
- SOD1
- TARDBP
- Others
- What to do in the clinic
Is ALS genetic?
- What have we learned from familial ALS?
- How heritable is sporadic ALS?
- Do we need a new model?
How common is familial ALS?
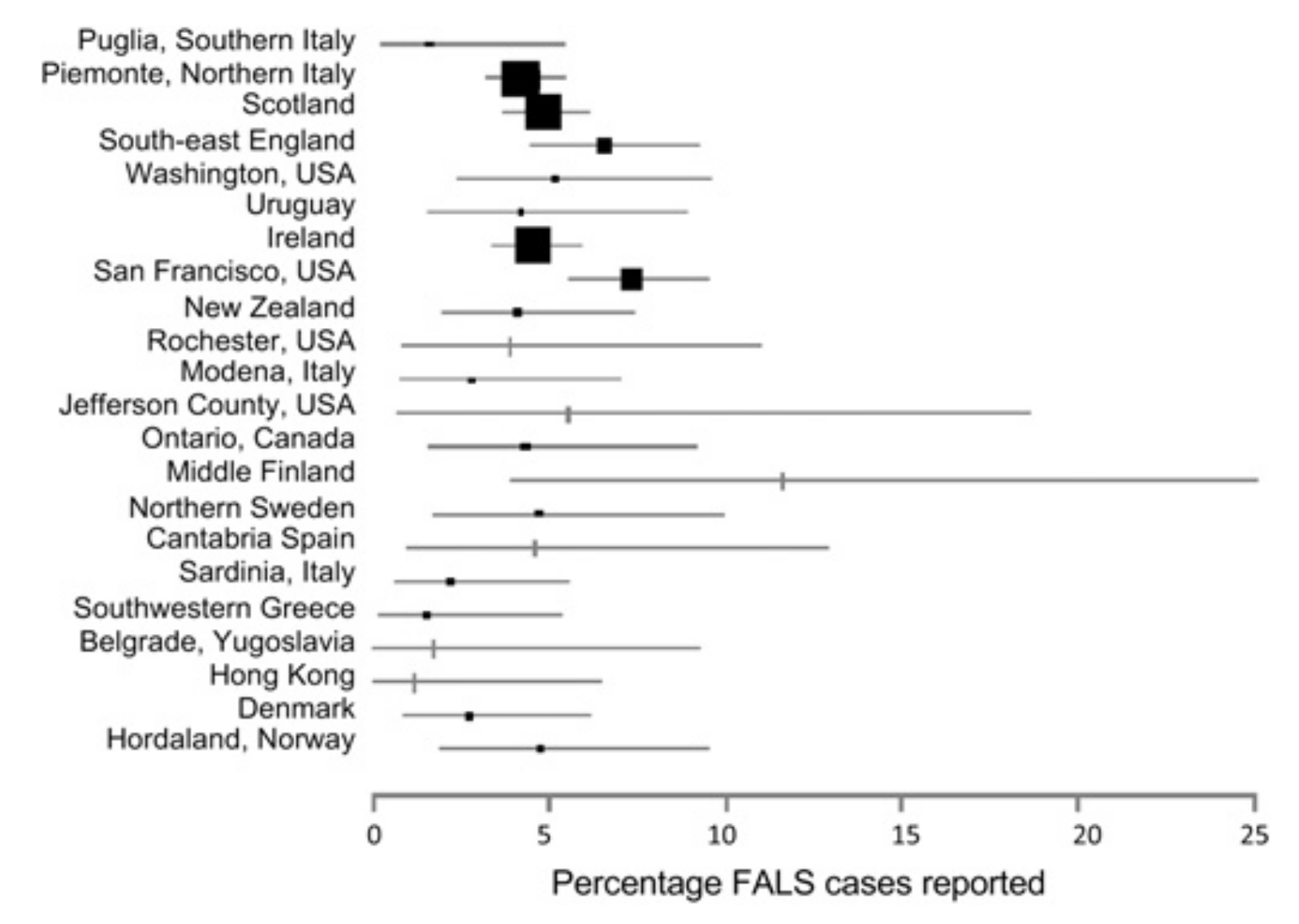
Byrne et. al. JNNP 2011.
doi
- Uncommon - 5-10%
- Geographically variable
- guesswork with family history
- clinical ALS only
- variable definition of familial
Limitations of older studies
Linkage studies in familial ALS have identified several key genes
SOD1
TARDBP
C9orf72
How heritable is sporadic ALS?
Twin studies - 60%
Al-Chalabi et. al. 2010 JNNP doi
Family pairs in Irish register
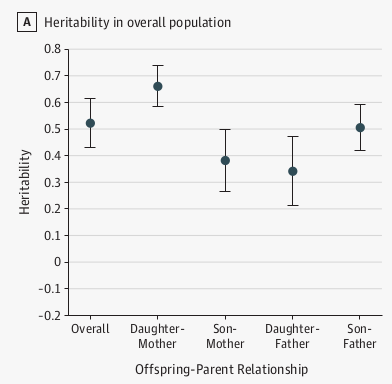 Ryan et. al. 2019 JAMA N doi
Ryan et. al. 2019 JAMA N doi
Germline monogenic causes only explain ~15% of apparently sporadic ALS
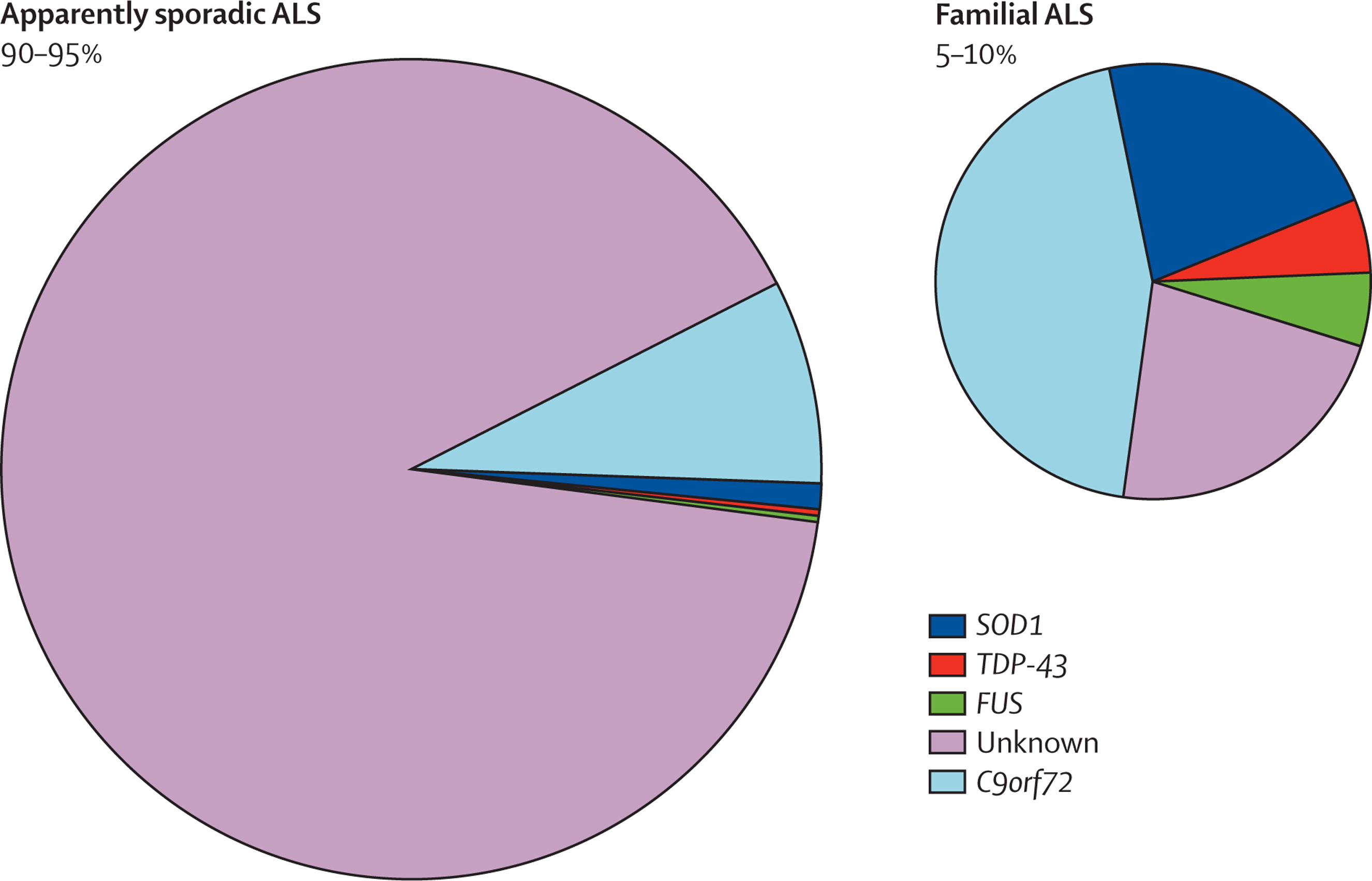
'Missing' heritability
Do we need a new model?
- Mutations are not equivalent
- Currently unknown non-genetic modifiers of penetrance and severity
structure
- Is ALS genetic?
- C9orf72
- SOD1
- TARDBP
- Others
- What to do in the clinic
C9orf72 hexanucleotide repeat expansion
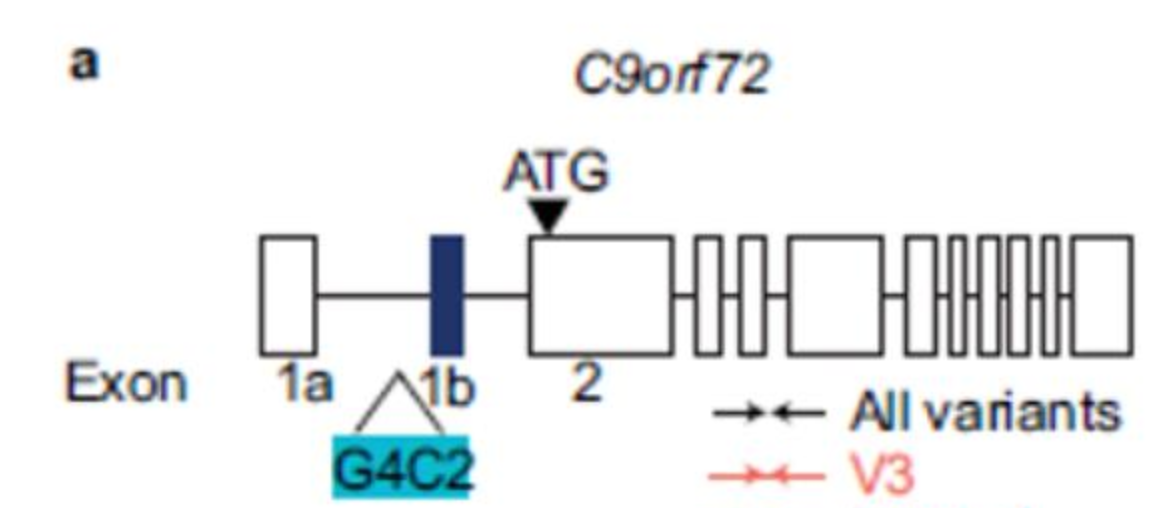
- >30 repeats, can be thousands
- Does not show anticipation
- Repeat length (in blood) does not correlate with clinical features
- Likely somatic repeat instability
Mechanism - controversial
- Loss of function - vesicle trafficking/autophagy?
- Toxic repeat RNA
- Toxic repeat proteins

Clinical features
- Heterogeneous - ALS, FTD, or ALS+FTD
- Emerging evidence - psychosis, bipolar, not cognitively normal before symptom onset
- Family history - dementia unspecified?
Penetrance
- High (>90%) in the context of targeted testing in ALS/FTD clinics
- Healthy individuals carrying this mutation - ?0.15% Beck 2013
- Several other case reports of healthy older adults >80. Would they remain healthy?
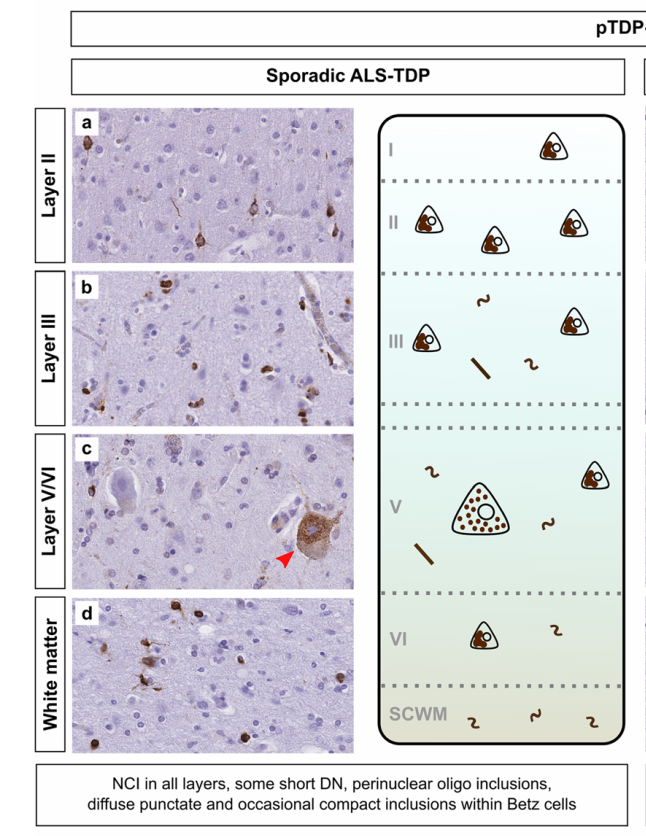
Neuropathology
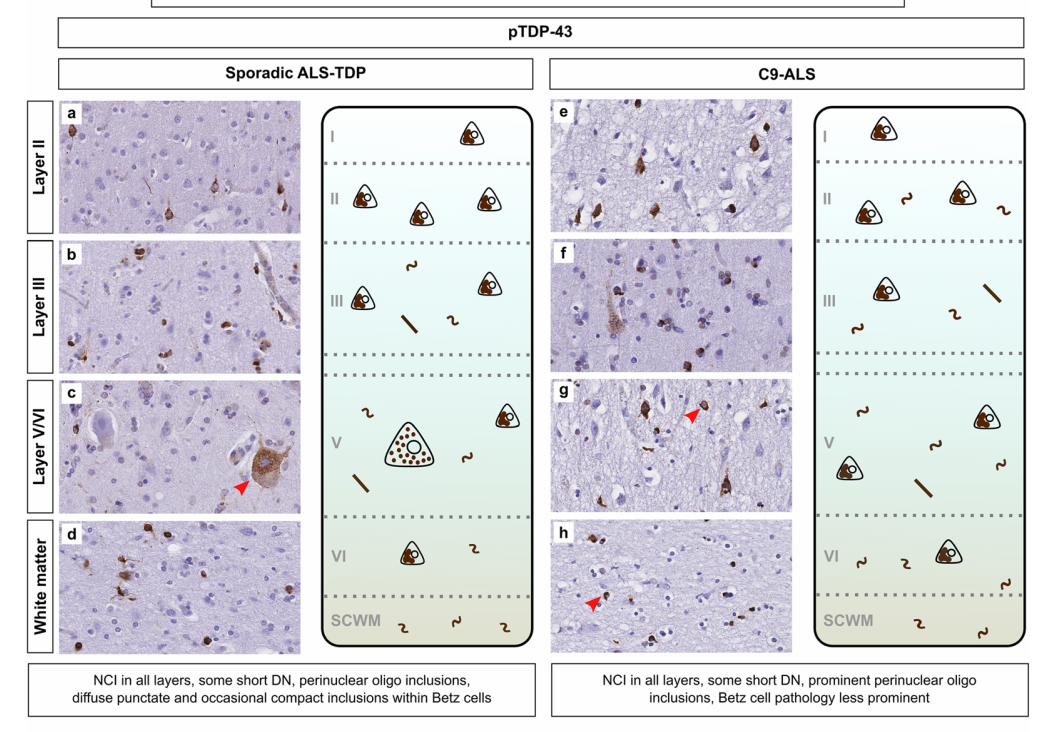
Similar (but not identical) distribution and morphology of TDP43 pathology to sporadic ALS.
Gene therapy trials in C9orf72
- Biogen trial - discontinued Mar 22
- No benefit, discontinued entire clinical program
- WAVE life sciences - ?recruiting since 2021 - Cambridge one site (Alex Murley)
- Need data published, huge scope for treatment refinement
SOD1
- Cu/Zn superoxide dismutase 1
- ~200 reported variants
- A4V - 50% in USA - aggressive course (survival 1y from diagnosis)
- heterozygous D90A - common polymorphism in Scandinavia - occasionally found in typical ALS
- homozygous D90A - slower disease course - up to 10y
- No FTD overlap
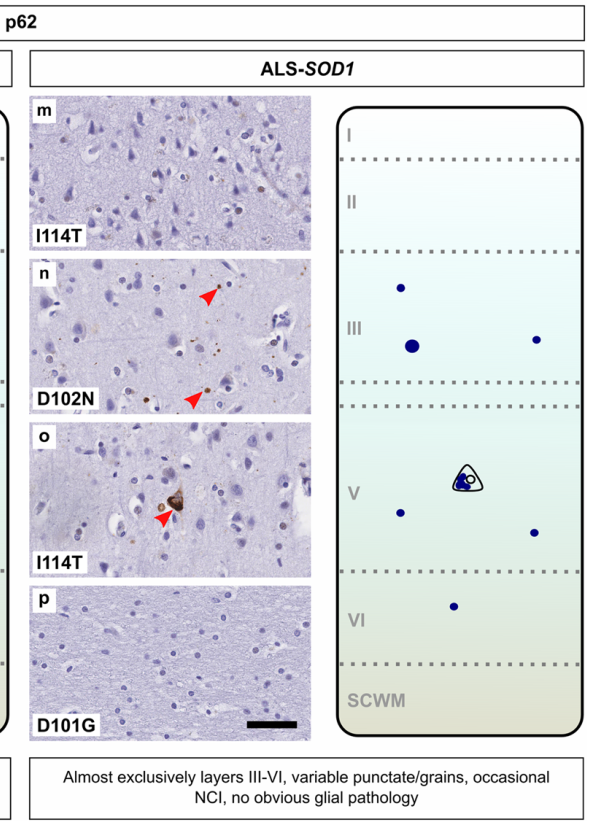
Neuropathology
- no TDP43
Tofersen - VALOR trial
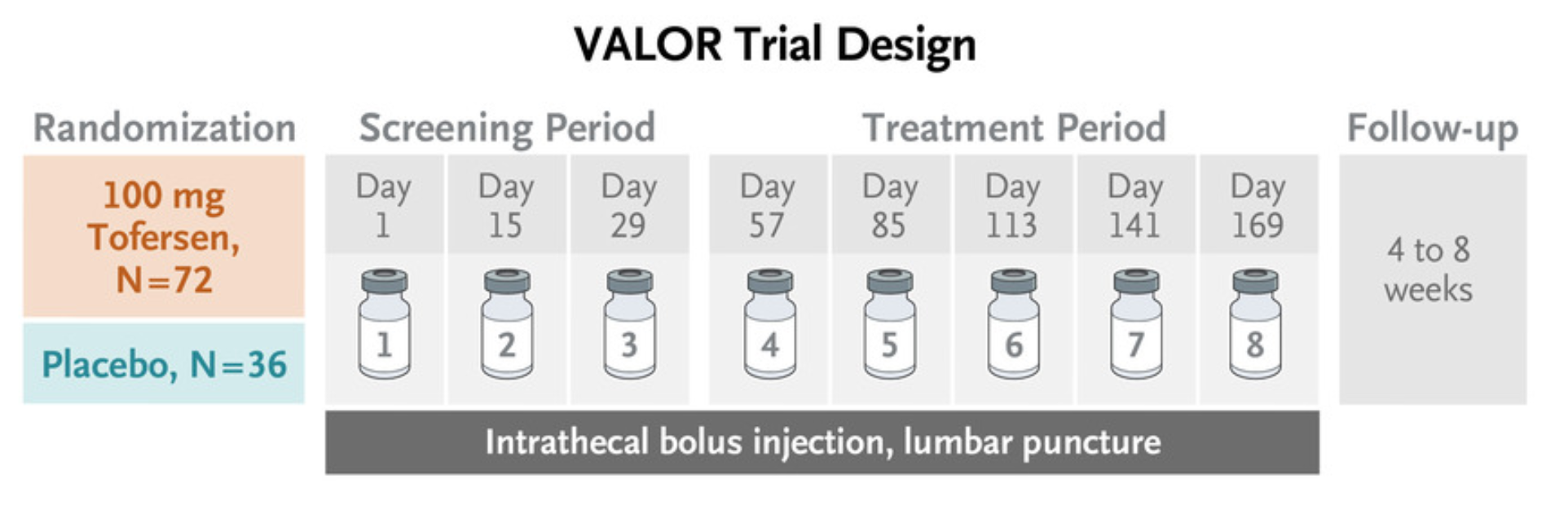
+ open-label extension
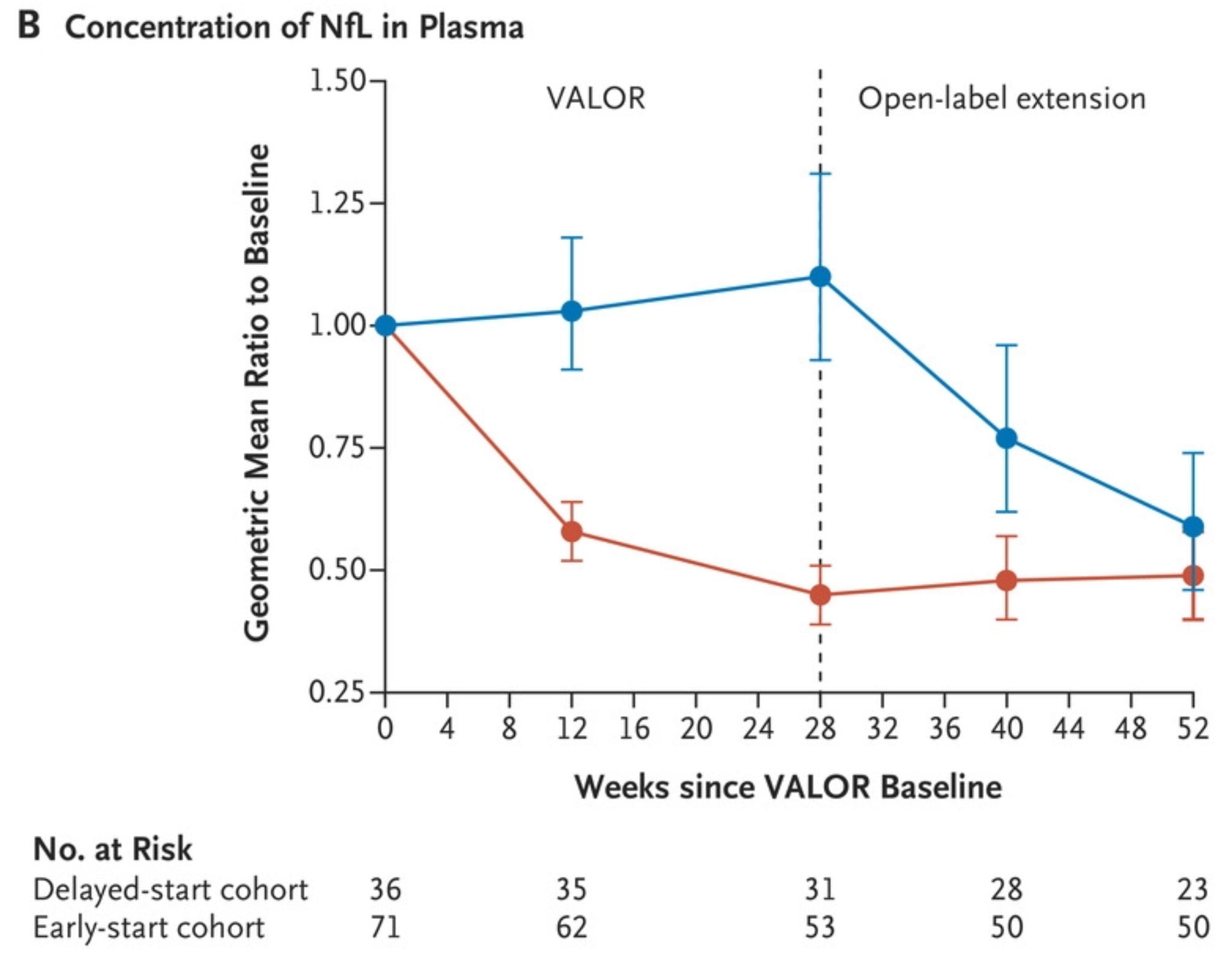
Neurofilament light
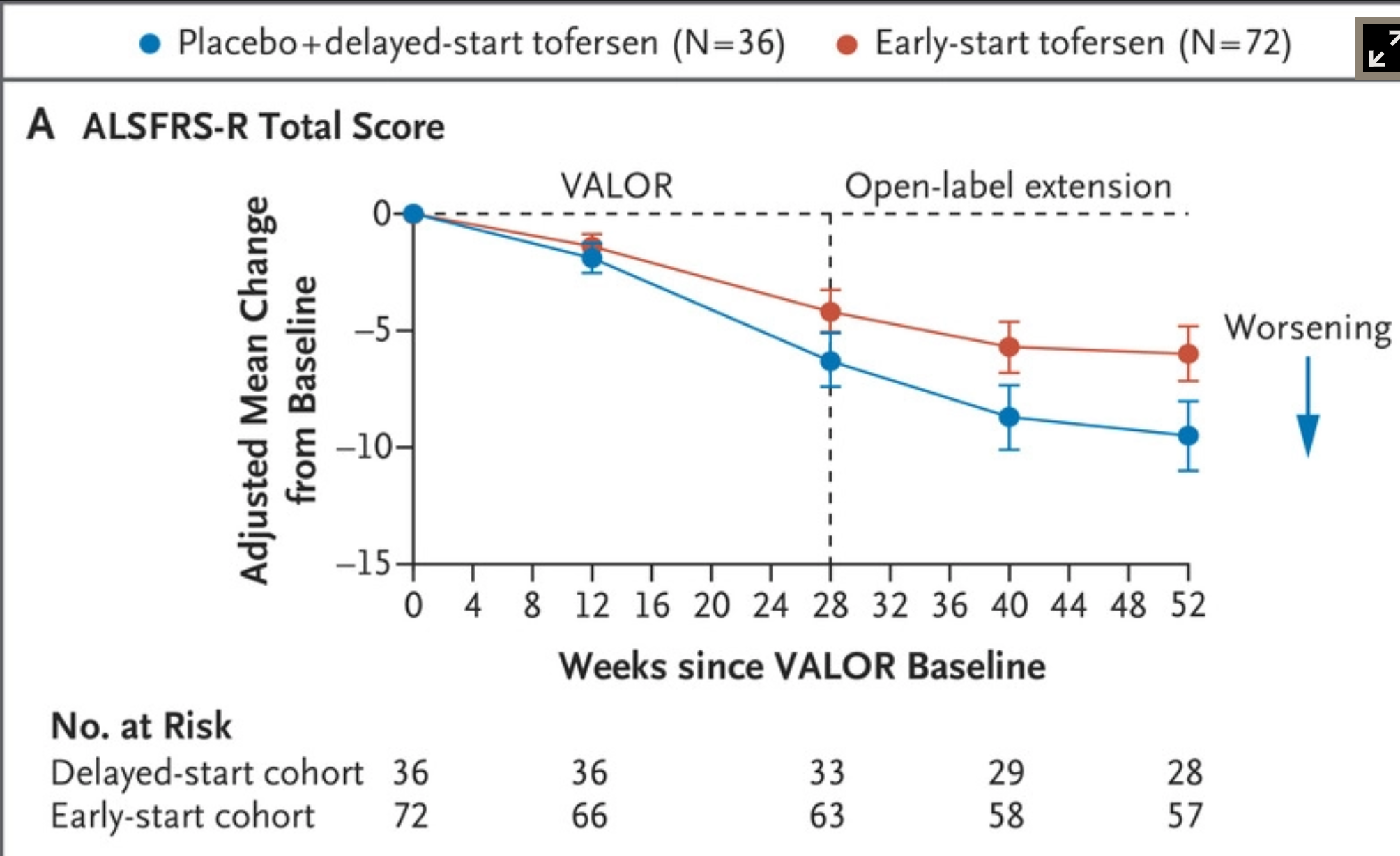
Functional rating scale
Trial limitations
- All SOD1 mutations included
- Did not meet primary endpoint
- Is suppressing all SOD1 (mutant and WT) a good idea?
- ATLAS trial in presymptomatic carriers of high-penetrance SOD1 mutations recruiting
TARDBP
- DNA binding protein
- FTD, ALS or FTD+ALS
- Why are TARDBP mutations an uncommon cause of genetic ALS?
TARDBP for modelling ALS
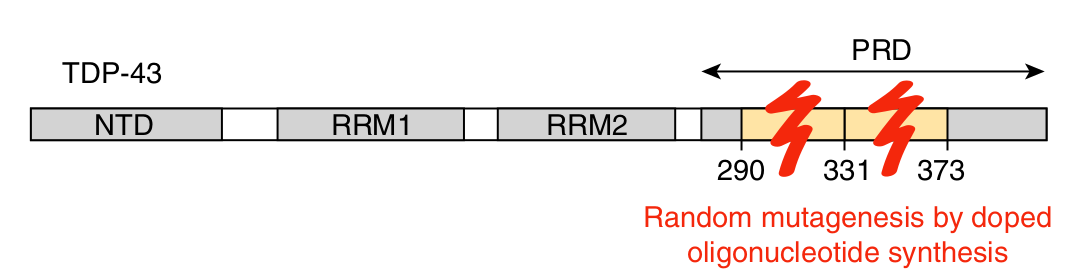
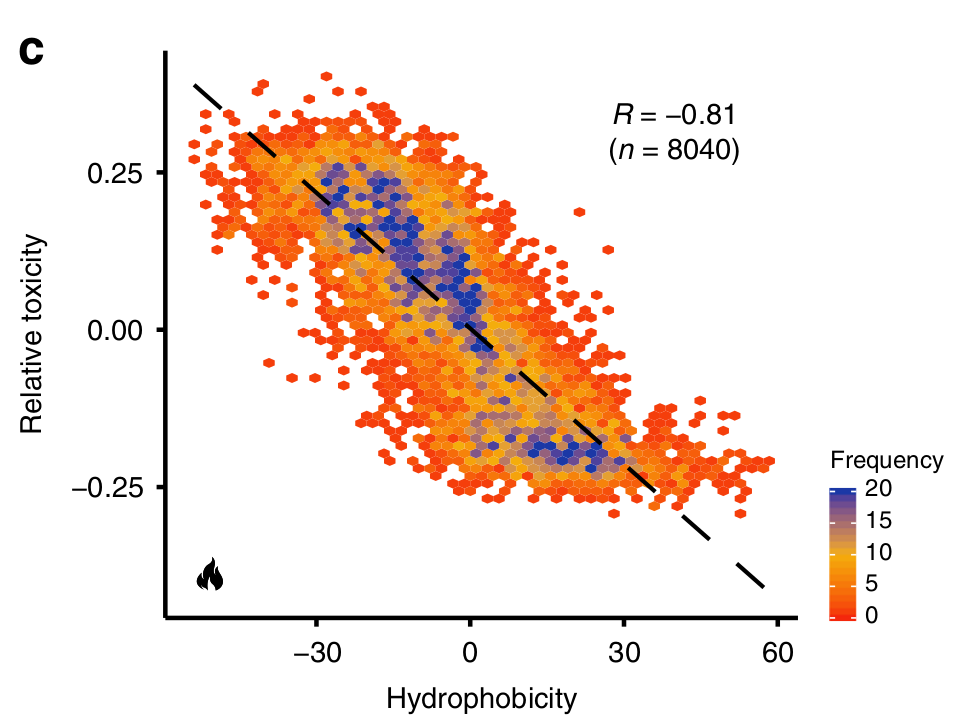
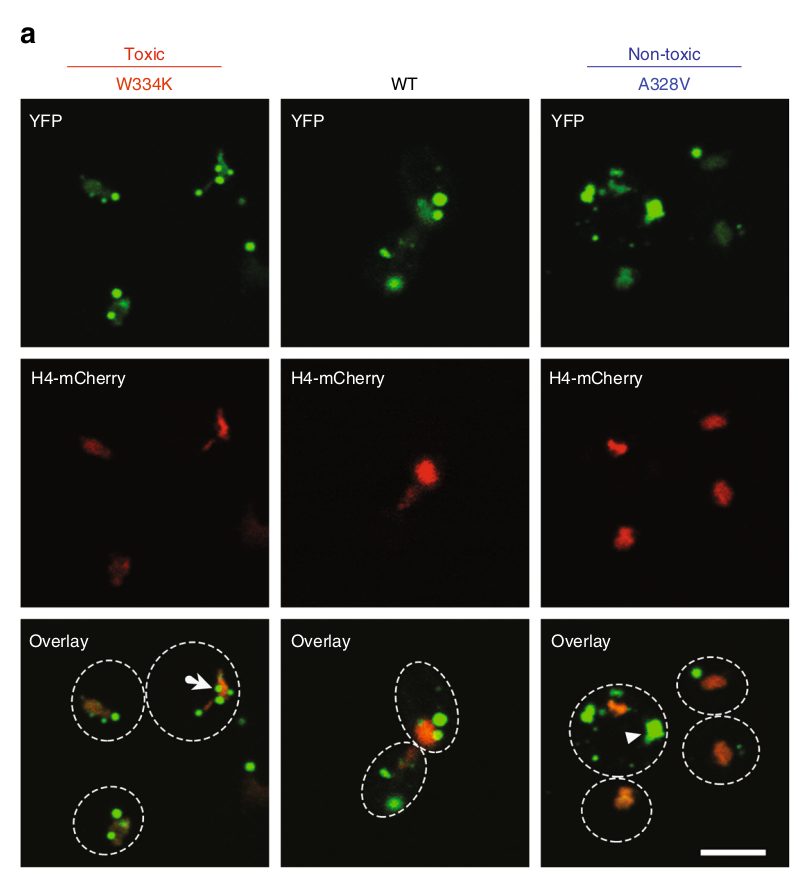
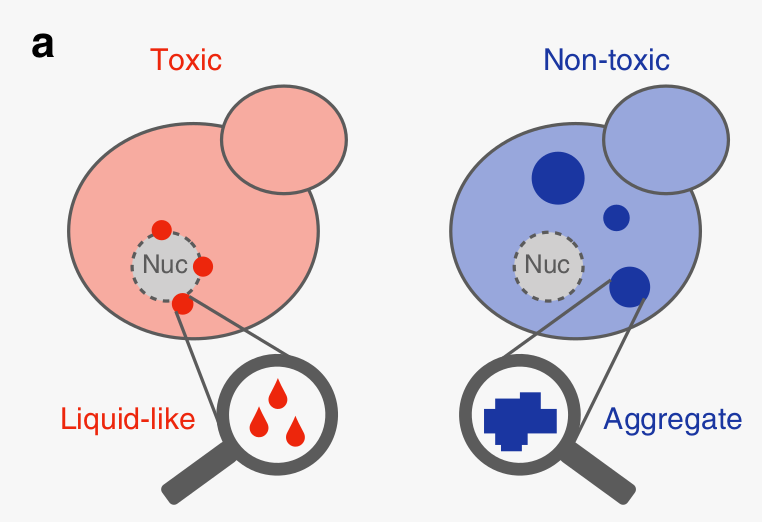
Bolognesi et. al. Nature Comm 2019 doi
FUS
- RNA binding protein
- Young onset, aggressive ALS
- essential tremor, FTD too?
- Cytoplasmic aggregates, but not TDP43
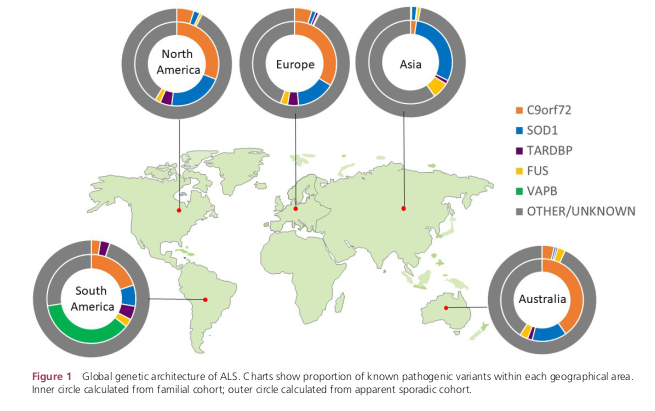
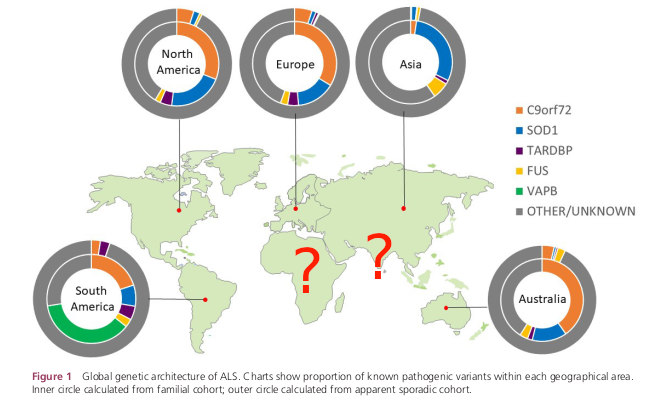
Geographic variation
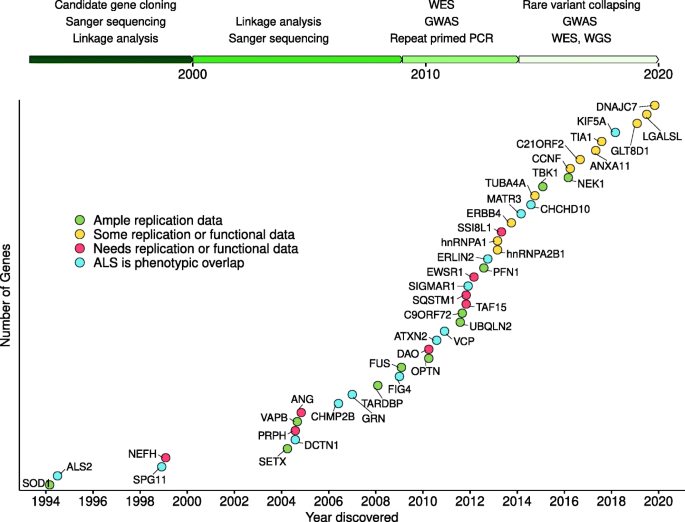
Other genes
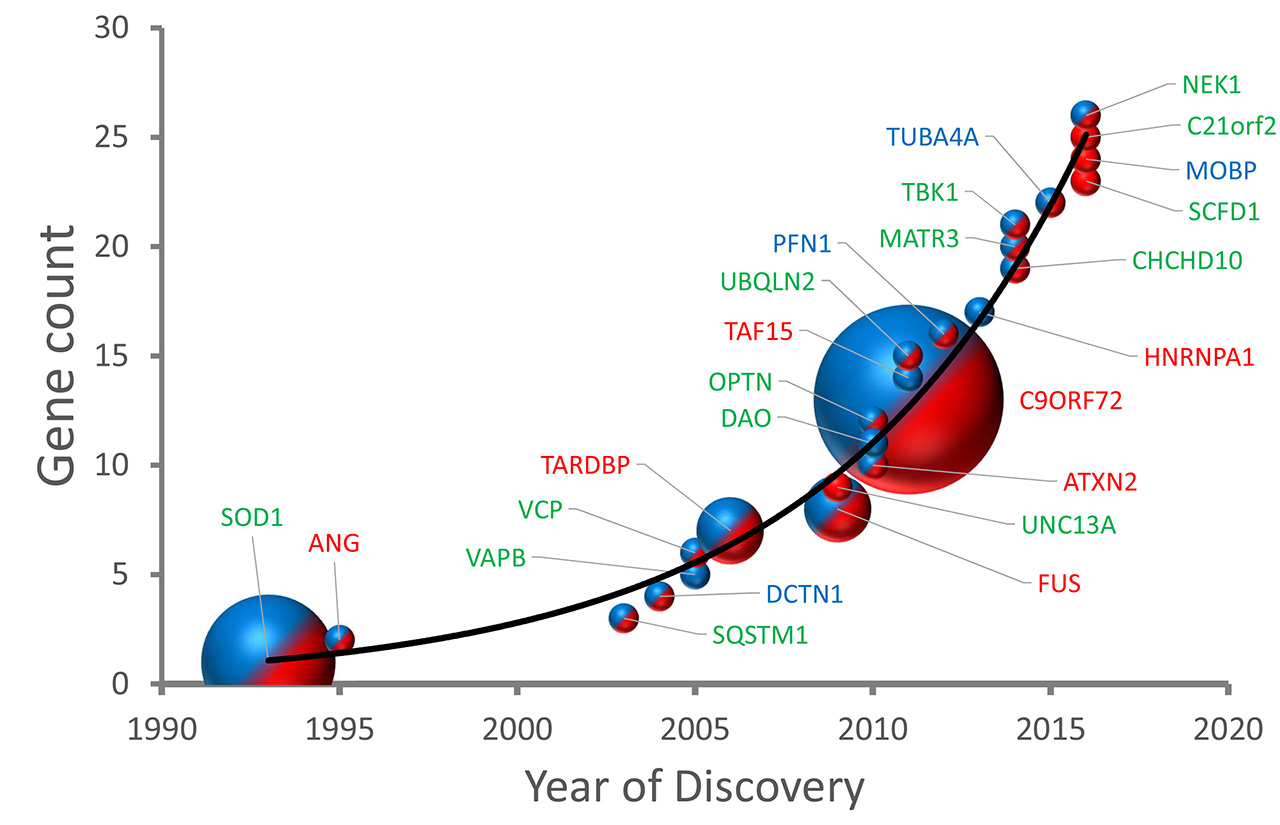
Optimistic view
GWAS
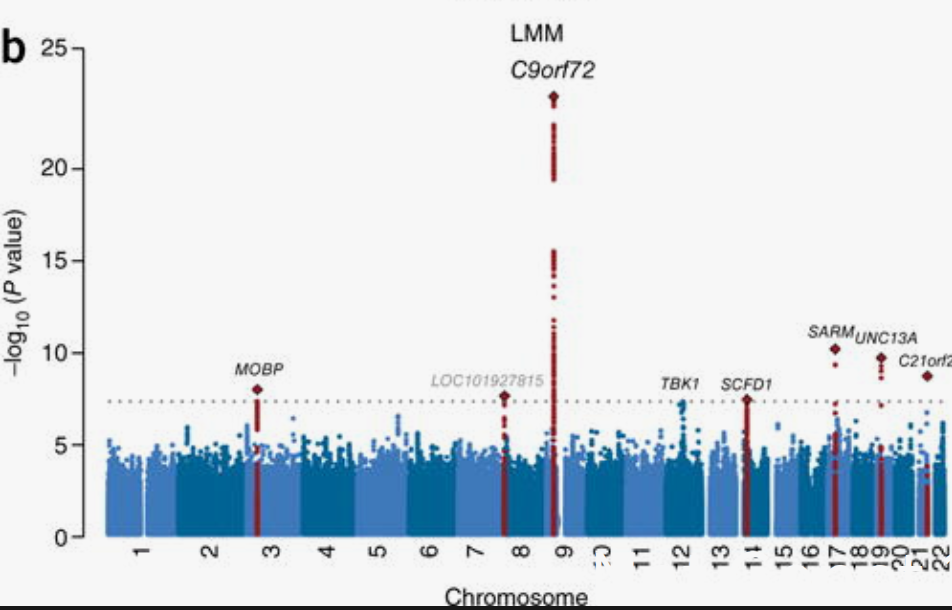
Relatively few *common* variants
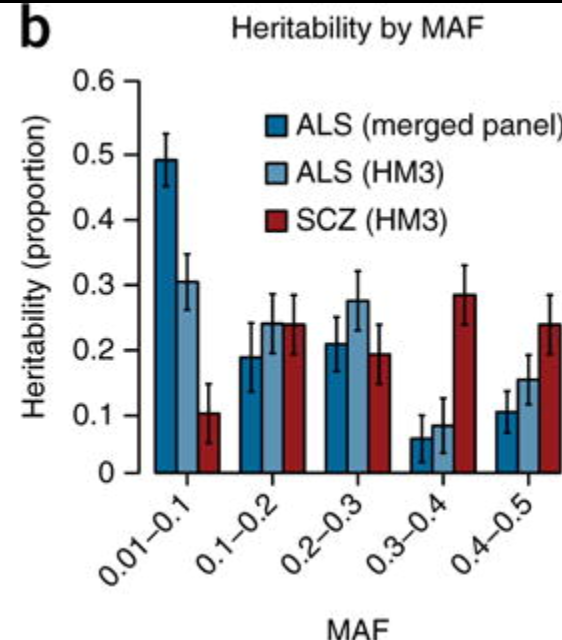
Rare variants may account for more heritability in ALS vs. schizophrenia.
Modelling ALS incidence as a multistep process
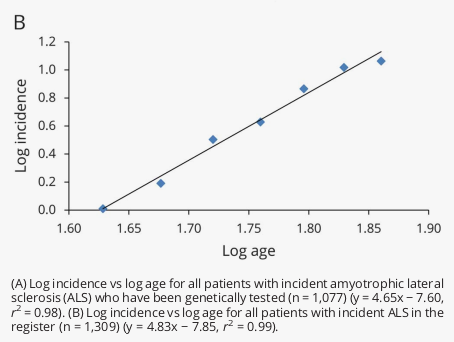
Sporadic ALS may be a 5 step process
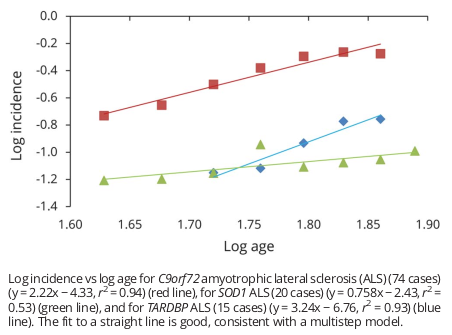
Genetic ALS may only be 2 or 3
structure
- Is ALS genetic?
- C9orf72
- SOD1
- TARDBP
- Others
- What to do in the clinic
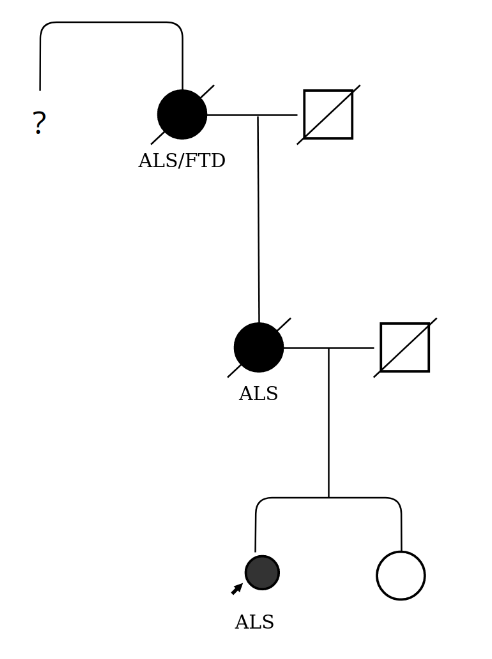
Cases
The two children of a patient with ALS without a wider family history accompany their parent (mother) to clinic. After routine discussion about the causes of ALS, the patient expresses a wish to have all known genetic causes excluded. One of the children becomes angry, saying not to do this as he does not want to find out that he is at an increased risk of getting the disease.
A 16-week pregnant woman with ALS without a family history requests rapid genetic testing to guide termina- tion if an ALS gene variant is found.
A 30-year-old patient with ALS but without a family history requests genetic testing and is found to have a C9ORF72 hexanucleotide repeat expansion. At a subsequent appointment, the patient is accompanied by both parents, who are asymptomatic.
A patient with ALS without a family history and with a lower motor neurone-predominant phenotype arranges private whole-genome sequencing, which reports a variant of uncertain significance in ABCD1. The patient is concerned that they have been misdiagnosed.
A patient with ALS without a family history and with a typical progression rate has read about gene-targeting trials in SOD1-mediated ALS. They request genetic testing so that they might be eligible to enrol. It reveals that they are heterozygous for a ‘likely pathogenic’ variant associated with a characteristically very slowly progressive, typically homozygous recessive form of ALS.
A patient with ALS without a family history and with a lower motor neurone-predominant phenotype arranges private whole-genome sequencing, which reports a variant of uncertain significance in ABCD1. The patient is concerned that they have been misdiagnosed.
Phenotype
- ALS remains largely a clinical diagnosis
- Spectrum - pure motor, pure cog, both
- Age of onset
- Rate of progression
- weak predictors
Family history
Not just ALS
- Lost weight, mobility/speech declined rapidly at end of life?
- Dementia - AD misdiagnosed?
- Alcohol abuse, bipolar, schizophrenia?
- Chestnuts - adoption, non-paternity, consanguinity
When to discuss genetics?
- Patient wants to know - Easier, may need specialist input
- Patient doesn't want to know - Difficult, clinical judgement
- Patient hasn't thought about it - Difficult, clinical judgement
- Research/clinical trial access
- With discretion/at patient request at diagnosis, mainly in followup
Other considerations
- Capacity - tricky - does mild impulsivity affect capacity?
- Family dynamics - beware the anxious healthy biological relative who has read up
Testing - ALS patients
- DNA storage
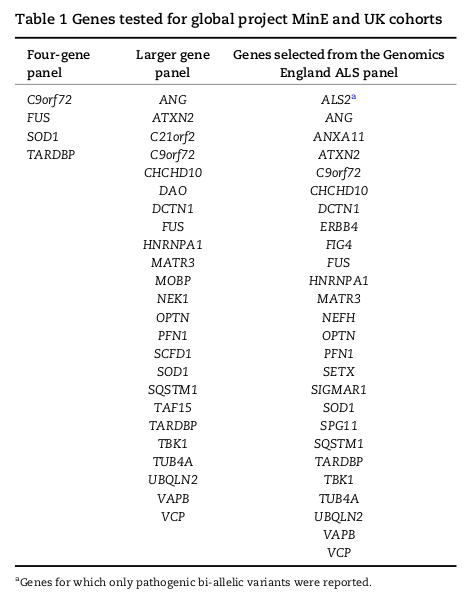
- Targeted genes
- Panel
- WGS virtual panel
R58
WGS considerations
- 433 entities - 97 green
- Many non-ALS genes
- Privacy and research participation
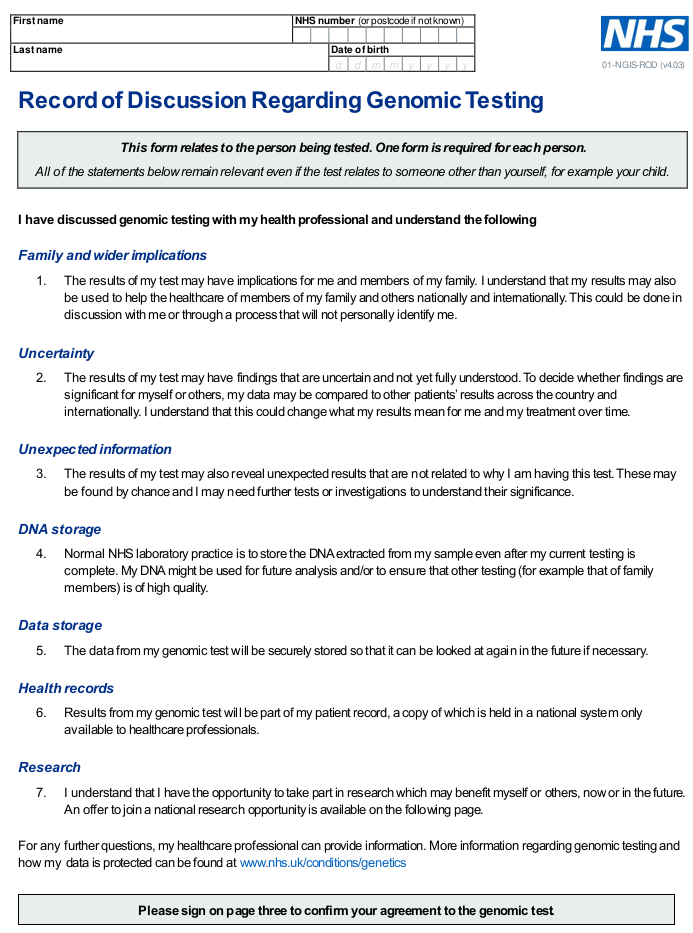
- Consent and recording
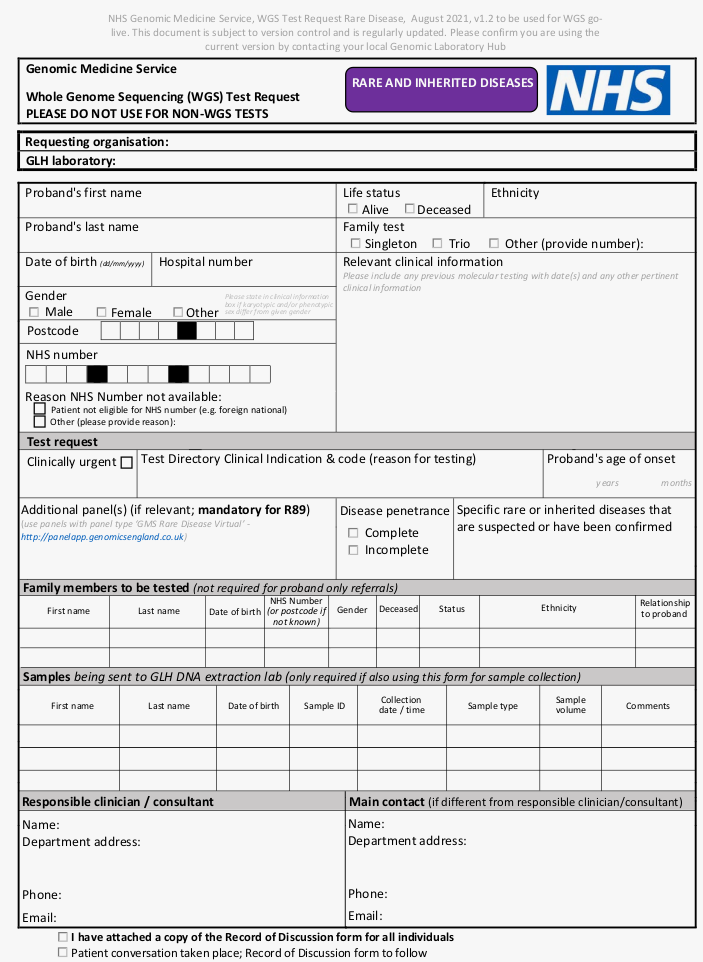
NHS genomics forms
Interpreting results
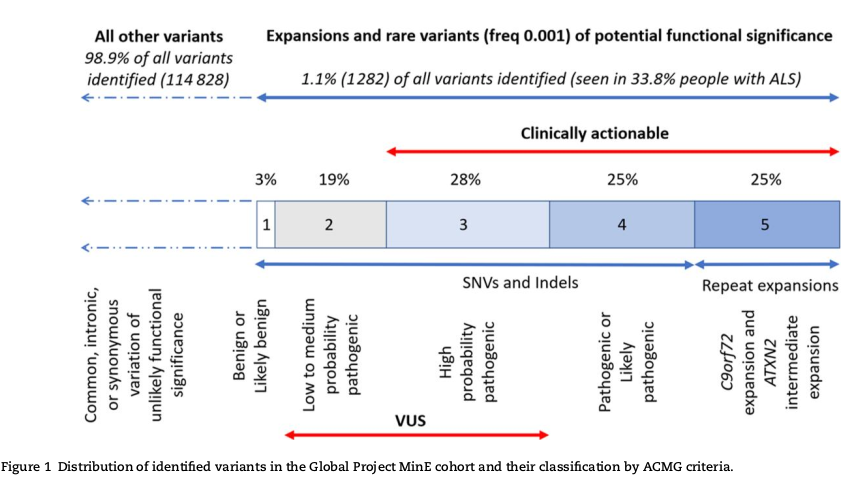
Example result
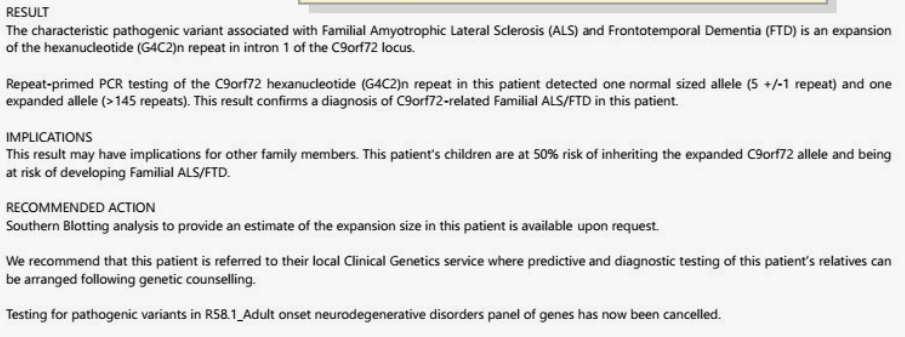
Disclosing genetic testing results
- Patients generally disclose once they have processed
- Patients can nominate relatives to have access to results after death
- Get genetics advice if patient refuses to disclose/otherwise believe at risk
- Occupational implications
- Health insurance - insurers can request Huntington's predictive test results
tl;dr
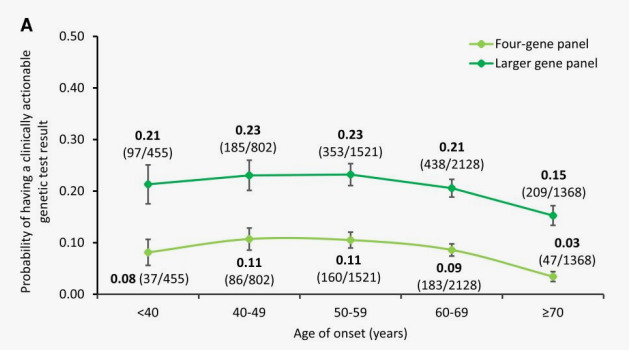
- "actionable" genetics in 10-20% of ALS
- This will likely increase in proportion and complexity
- Genetics can be discussed with all ALS patients
- Testing is evolving - locally we use WGS virtual panel
- Thought/care with results
- Specialist ALS/FTD and genetics services exist
structure
- Is ALS genetic?
- C9orf72
- SOD1
- TARDBP
- Others
- What to do in the clinic